本文链接:https://www.yuque.com/gs123/share/magnesium
说明:
- 本文涉及的任何观点均不构成任何临床治疗建议,请咨询医生!
- 本人不是医生,以下错误之处,还请读者(特别是医学专业人士)不吝指正,谢谢。
门冬氨酸镁(门冬氨酸钾镁片 magnesium aspartate)
国内医院没有单独的口服补镁剂,口服补镁一般都是使用门冬氨酸钾镁片,这是门冬氨酸钾+门冬氨酸镁的混合物。
口服门冬氨酸钾镁中镁的剂量小,是否也与长期的低钾不能纠正有关,试改用氯化镁或其他药物是否对低血钾的长期纠正有帮助值得观察
家族性Gitelman综合征诊治经验;2015 doi:10.3760/cma.j.issn.1000-6699.2015.12.010 ;中山大学附属第一医院 内分泌科
目前国内大多数采用门冬氨酸钾镁片,对于补镁后,仍无法纠正低钾症状的患者,治疗以补钾、保钾为主,还可选用醛固酮受体阻断剂如安体舒通(螺内酯)、远曲小管氯化钠转运阻滞剂如氨苯蝶啶以及血管紧张素转换酶、血管紧张素受体拮抗剂等,但运用以上药物需注意监测血压,避免低血压……患者目前服用氯化钾缓释片 9.0g/d,门冬氨酸钾镁 9片 /d,螺内酯 20mg/d,氨苯蝶啶50mg/d,长期随访该患者发现,在规范服用以上药物的情况下,约 2~3个月便有四肢抽搐发作,需至当地医院静滴氯化钾约 2g连续 4~5d,症状可缓解。与文献报道比较,本例患者低钾更难纠正,极易复发,临床症状明显,除与性别因素相关外,SLC12A3 基因439th aa G(S)和 615th aa S(/L)的复合杂合突变可能是该患者病情难治的原因。
难治性 Gitelm an综合征 1例及临床诊疗体会;2016 DOI: 10.3969/j.issn.1005-8982.2016.06.029 ;广东省中医院
case1:纯合GS,18岁,男;伴精神分裂症(疑似)
用药:
- 氯化钾缓释片:3g/天
- 门冬氨酸钾镁片:0.3g/天
- 螺内酯:40mg/天
- 帕潘立酮:治疗神经分裂,用量未知,半年减量至停用
效果:
- 血钾:2.99 —-> 3.2~3.5
- 血镁:0.49 —-> 0.57~0.67
An 18-year-old male……His electrolyte disturbances were thought to be caused by acute psychosis and were expected to recover soon, the patient was discharged with oral potassium and magnesium supplementations.
During the regular following up, the patient felt a little fatigue as before while his psychosis maintained complete remission. Two weeks later after discharge, laboratory studies showed worsened hypokalemia (2.99 mmol/L) and hypomagnesemia (0.49 mmol/L) despite potassium and magnesium supplementations…..A homozygous mutation of exon 23 in the SLC12A3 gene which led to p.Arg896Gln….Eventually, the diagnosis of GS was established.
Thus, additional spironolactone 螺内酯 (40 mg/day) combined with increased doses of oral potassium chloride sustained-release tablets (3.0 g/day) and potassium magnesium aspartate (门冬氨酸钾镁片) (0.3 g/day) were administered. During next half a year, fatigue resolved, paliperidone gradually tapered and eventually discontinued while psychosis maintained complete remission. His serum potassium was near normal (3.2–3.5 mmol/L), hypomagnesemia significantly improved (0.57–0.67 mmol/L).
Schizophrenia-like psychosis and gitelman syndrome: a case report and literature review Doi: 10.1186/s40064-016-2579-5; 浙二医院,潘冰(神经内科),牟利军(肾内)等;2016
Case2:复合杂合GS,62岁,男;30年病史 + 10年2型糖尿病史
用药:
- 螺内酯:20mg x 每天2次
- 门冬氨酸钾镁片:2片 x 每天3次
效果:
- 血钾:2.8~3.1(最低1.84)—-> 随访3.5+(4.05 出院时)
- 血镁:随访0.6+ (0.78 出院时)
A 62-year-old Chinese man……The patient’s weakness in the extremities started 30 years ago, but spontaneously recovered in one week after each instance. 20 years ago, he was admitted to the hospital because of difficulty walking upstairs and a diagnosis of hypokalemia was made. The patient’s symptoms quickly improved with potassium replacement therapy. Despite any medicine treatment, his serum potassium levels ranged from 2.8 to 3.1 mmol/L in the past 10 years. He had consumed liquorice甘草 water daily for seven days prior to admission……The past medical history revealed only type 2 diabetes mellitus since the age of 52. For that reason, he was treated with 10 mg of dapagliflozin and 25 mg of alogliptin daily.
Partial electropherograms from exon 10 and exon 21 of the SLC12A3 gene showing two heterozygous missense mutations in the patient. A and B: One is from G to A at nucleotide position 1567 [NM_000339, c.1567G>A; p.Ala523Thr] (A), and the other is from G to A at nucleotide position 2542 [NM_000339, c.2542G>A; p.Asp523Asn] (B).
The patient’s signs and symptoms improved with potassium replacement therapy (10 g of potassium chloride injection daily), hydration, and discontinuation of liquorice ingestion. His serum potassium was increased to normal within 5 days. Correspondingly, CK decreased to normal within 8 days. Moreover, the ECG returned to normal on the third hospital day. Five weeks later, the patient was started on antisterone (20 mg, po, bid) and potassium magnesium aspartate tablets (2 tablets, po, tid), following the SLC12A3 gene results. Upon follow-up at 3 mo, the levels of CK, MYO, and potassium remained normal and magnesium was above 0.6 mmol/L.
| Parameter | before treatments | after treatments | Reference range |
|---|---|---|---|
| Potassium (mmol/L) | 1.84↓ | 4.05 | 3.5-5.5 |
| Sodium (mmol/L) | 144 | 138 | 137-147 |
| Chlorine (mmol/L) | 98↓ | 99 | 99-110 |
| Magnesium (mmol/L) | 0.68↓ | 0.78 | 0.75-1.02 |
| pH | 7.47↑ | 7.40 | 7.35-7.45 |
| HCO3- (mmol/L) | 32↑ | 24 | 21-26 |
| Urinary pH | 8.0↑ | 6.0 | 5-6 |
Liquorice-induced severe hypokalemic rhabdomyolysis with Gitelman syndrome and diabetes: A case report. DOI: 10.12998/wjcc.v7.i10.1200;山西医科大学附属第一医院 内分泌科,2019
氧化镁(magnesium oxide)
Case3:复合杂合,55岁,女,英国
用药:
- (55-60岁)氧化镁:16mmol/天
- (60-62岁)门冬氨酸镁:40 mmol/天
- 螺内酯:100 mg/天
- 氯化钾:用量未知
效果:
- (55-60岁)血镁:0.5-0.6
- (60-62岁)血镁:0.6-0.75
A 55-year-old lady… was commenced on oral potassium and magnesium supplements (氧化镁magnesium oxide 16 mmol/day) together with spironolactone(螺内酯) 100 mg daily as a long term treatment. Molecular genetic analysis confirmed GS with the identification of compound heterozygous mutations inSLC12A3 (p.Arg209Gln and p.Ser615Leu)5. Despite oral supplementation, serum magnesium levels remained low (0.5–0.6 mmol/L)…….At 60 years of age…Oral magnesium supplementation was changed to magnesium aspartate门冬氨酸镁 and increased to 40 mmol/day in an attempt to normalise serum magnesium levels and prevent progression of the chondrocalcinosis and improve symptoms. From 60 to 62 years of age the serum magnesium has been maintained at near normal levels (0.6–0.75 mmol/L 血镁升高了) with improvement of musculoskeletal symptoms and no progression of any functional deficit in hand movements。
Case Report: Cervical chondrocalcinosis as a complication of Gitelman syndrome;2016 doi: 10.12688/f1000research.8732.1;英国Newcastle University
Case4:25岁,孕妇,美国
用药(孕期第10周,口服):
- 氧化镁:60 mmol/天(* Mg2+: 1 mEq = 1/2 mmol)
- 氯化钾:60 mmol/天(* K+:1 mEq = 1 mmol)
效果:
- 血镁 < 0.42 mmol/L ;血钾 <3 mmol/L
- 因口服效果无法达到理想值,之后改为静脉滴注氯化钾+硫酸镁(每周3次,后增加到每天一次),效果改善(血钾 2.5~3.3,血镁 0.7~1.0)。28周,破腹产,636克婴儿,存活
(第五次怀孕,之前3次自然流产,1次死胎…阿弥陀佛)A 25-year-old woman with GS presented at 6 weeks gestation with asymptomatic hypokalemia and hypomagnesemia. This was her fifth pregnancy. The prior pregnancies had been unsuccessful with the first three resulting in spontaneous abortion before 20 weeks and the fourth pregnancy complicated by fetal demise at 23 weeks. Her initial diagnosis of GS was made after the first pregnancy based on clinical presentation and laboratory data. Pre-pregnancy, she was maintained on oral electrolyte replacement.
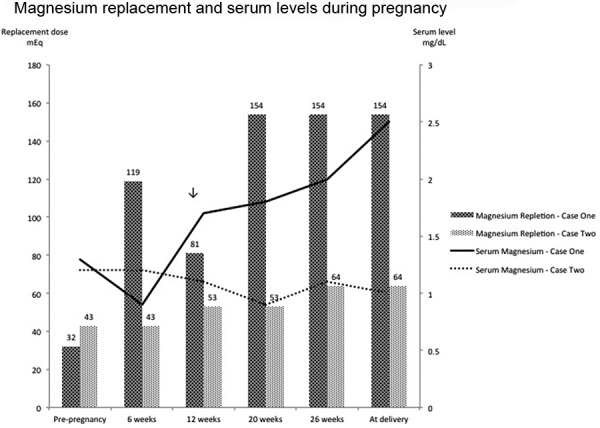
Late into her first trimester she became symptomatic with three separate emergency room visits for abdominal cramping. Symptoms of nausea, vomiting, perioral paresthesias, and tetany were absent. Electrocardiogram was normal. At 10 weeks gestation, on an oral regimen of 60 mEq of potassium chloride and 2,400 mg (119 mEq) of magnesium oxide per day, she was unable to maintain serum potassium levels greater than 3 mEq/L and serum magnesium levels greater than 1 mg/dL. Due to her clinical symptoms, laboratory data, and prior failed pregnancies in the setting of electrolyte derangements, she was started on thrice-weekly intravenous (IV) potassium and magnesium supplementation, as an outpatient at a local hospital, in addition to her oral regimen. Nephrology was then consulted to further guide management of her care.
Despite her aggressive oral regimen and thrice weekly IV supplementation she was unable to maintain a serum potassium greater than 3 mEq/L and a serum magnesium greater than 1.5 mg/dL. Outpatient, continuous IV electrolyte supplementation was started at 13 weeks gestation. Home health care services were arranged. She was started on a 24-hour infusion of magnesium and potassium. Initial dose of magnesium was 10 g of magnesium sulfate and 20 mEq potassium chloride. The electrolyte solution was reconstituted in 240 mL of normal saline and infused at a rate of 10 mL/h via continuous pump through a peripherally inserted central catheter. The patient had labs monitored initially twice a week and then once a week, with continuously increased doses of electrolyte solutions (Figure 1, Figure 2). With this regimen she was able to maintain serum potassium of 2.5 – 3.3 mEq/L, and serum magnesium of 1.7 – 2.5 mg/dL (normal lab range 1.6 – 2.6 mg/dL), close to our previously defined targets. Her maximum repletion requirements were 120 mEq of IV potassium and 19 g (154 mEq) of IV magnesium sulfate per day. At 28 weeks gestation, due to severe intrauterine growth restriction and reversed end-diastolic placental flow, she was hospitalized and delivered via cesarean section a viable, 636 g infant.
Two cases of successful pregnancy in patients with Gitelman’s syndrome,2015 doi: 10.5414/CN108526,Division of Nephrology, Vanderbilt University Medical Center,美国·田纳西州
氯化镁(magnesium chloride)
Case5:10岁,女,中国,湘雅儿科
该病目前治疗上仍以对症治疗为主。轻度以饮食调整为主;中度可考虑口服氯化钾及氯化镁;重度建议静脉给药。需注意的是,除补充钾离子及镁离子外,根据血清电解质结果需适当补充氯化钠。
Gitelman综合征伴体格发育落后1例;2017 doi: 10.11817/j.issn.1672-7347.2017.10.019;中南大学湘雅医院儿科
Case6:37,42岁,姐妹,中国,中山大学附一内分泌
Gitelman综合征患者血镁正常并不罕见,因长期慢性缺镁,患者血清镁可能正常,但细胞、肌肉、骨骼等贮备镁通
常缺乏。镁作为Na-K-ATP酶激活剂,能促使细胞外液钾进入细胞内,同时作为钾在细胞内滞留,增加钾流出。所以补镁有助于升钾,即使在血清镁不低时。高剂量的硫酸镁引起腹泻,而氯化镁的耐受性相对较好。推荐氯化镁4~5 mg·kg~·d。1分为3~4次服用,防止腹泻…… (此段,引用的文献=DOI: 10.1093/qjmed/hcq123)
家族性Gitelman综合征诊治经验;2015 doi:10.3760/cma.j.issn.1000-6699.2015.12.010 ;中山大学附属第一医院 内分泌科
Case7:34~35岁,孕妇,美国
用药:
- (第一胎,34岁)氯化镁:26.5 mmol/天
- (第二胎,35岁)氯化镁:32 mmol/天
- (第一/二胎)氯化钾:200 mmol/天
效果:
- (第一胎,34岁)血钾 3.6,血镁 0.41:第7周+6天,胎儿死亡
- (第二胎,35岁)血钾 3.2,血镁 0.41~0.45;33周,破腹产,健康婴儿
The second patient is an otherwise healthy 34-year-old woman referred to nephrology for evaluation of hypokalemia and hypomagnesemia. She was diagnosed with GS after presenting with a serum potassium of 2.6 mEq/L, serum magnesium of 0.9 mg/dL, metabolic alkalosis, modestly low blood pressure, and additional testing that revealed an elevated urine potassium and chloride, increased fractional excretion of magnesium, hypocalciuria, and negative diuretic screen. Interestingly, she had been maintained on an oral contraceptive pill containing drospirenone until shortly prior to her initial presentation for hypokalemia. Genetic testing was not pursued.
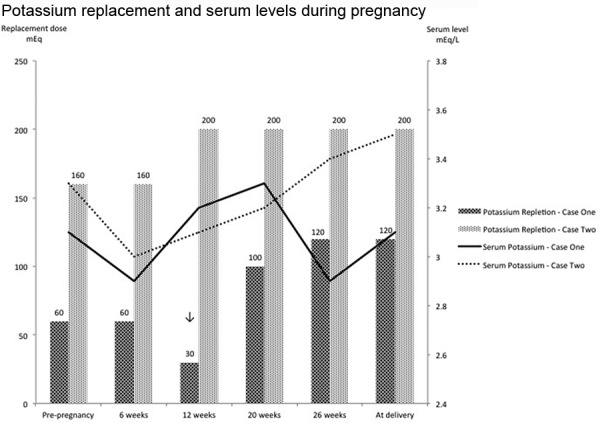
One year later, at the time of her first pregnancy, she presented with serum potassium and magnesium levels of 2.9 mEq/L and 1.4 mg/dL, respectively. Her oral repletion was increased to 200 mEq/day of potassium chloride and 640 mg/day (53 mEq) of magnesium chloride. Spontaneous fetal demise occurred at 7 weeks and 6 days. Her serum potassium and magnesium levels were 3.6 mEq/L and 1.0 mg/dL at the time of this event.
She became pregnant again 1 year later. At the time of her second pregnancy, oral potassium and magnesium replacement were increased from pre-pregnancy doses of potassium chloride 160 mEq/day and magnesium chloride 512 mg/day (43 mEq) to potassium chloride 200 mEq/day and magnesium chloride 768 mg/day (64 mEq). Serum potassium and magnesium levels were monitored at 3-week intervals throughout the pregnancy. Goal levels were achieved with a serum potassium of ~ 3.2 meq/L and serum magnesium levels greater than 1.0 – 1.1 mg/dL (normal lab range 1.5 – 2.5 mg/dL). She was asymptomatic throughout her pregnancy and her electrocardiogram was unremarkable. She delivered a healthy infant at 33 weeks gestation via cesarean section.
Two cases of successful pregnancy in patients with Gitelman’s syndrome,2015 doi: 10.5414/CN108526,Division of Nephrology, Vanderbilt University Medical Center,美国·田纳西州
Case A(下图中case one),B(下图中case two) 两个病例的用药及血钾/血镁水平对比
 |
 |
|---|---|
| Figure 1. Magnesium supplementation (depicted by the bar graph) and corresponding week during pregnancy (dose in mEq is given above each bar). Serum magnesium levels (depicted by the line graph) and corresponding week during pregnancy. Downward arrow indicates patient 1’s transition from oral to intravenous supplementation. |
Figure 2 Potassium supplementation (depicted by the bar graph) and corresponding week during pregnancy (dose in mEq is given above each bar). Serum potassium levels (depicted by the line graph) and corresponding week during pregnancy. Downward arrow indicates patient 1’s transition from oral to intravenous supplementation. |
Case8:55~62岁,女,英国
A 55-year-old lady… was commenced on oral potassium and magnesium supplements (氧化镁magnesium oxide 16 mmol/day) together with spironolactone(螺内酯) 100 mg daily as a long term treatment. Molecular genetic analysis confirmed GS with the identification of compound heterozygous mutations inSLC12A3 (p.Arg209Gln and p.Ser615Leu)5. Despite oral supplementation, serum magnesium levels remained low (0.5–0.6 mmol/L)…….At 60 years of age…Oral magnesium supplementation was changed to magnesium aspartate门冬氨酸镁 and increased to 40 mmol/day in an attempt to normalise serum magnesium levels and prevent progression of the chondrocalcinosis and improve symptoms. From 60 to 62 years of age the serum magnesium has been maintained at near normal levels (0.6–0.75 mmol/L 血镁升高了) with improvement of musculoskeletal symptoms and no progression of any functional deficit in hand movements。
Case Report: Cervical chondrocalcinosis as a complication of Gitelman syndrome;2016 doi: 10.12688/f1000research.8732.1;英国Newcastle University
Case9:34岁,女,日本
We report a 34-year-old woman with muscle weakness and tetany/seizures caused by electrolyte imbalance…….She had 2 heterozygous mutations in the SLC12A3 gene, one of which has been reported previously as a GS disease-causing mutation (c.1732G>A, p.Val578Met).[13] The other heterozygous mutation (c.2537_38delTT, p.846fs) has not been previously reported (Fig. (Fig.11).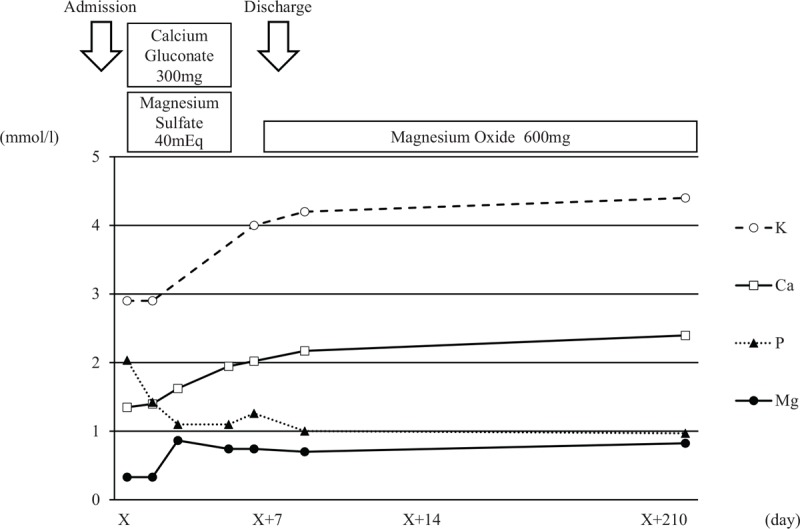
Clinical course of GS patient. Supplementation therapy of calcium gluconate and magnesium sulfate infusion was tapered within 2 days of admission. Electrolyte imbalance during oral administration of a low dose of magnesium oxide was within the normal range after discharge.
Gitelman’s syndrome with hyperphosphatemia, effectively responding to single oral magnesium oxide administration: A case report. DOI: 10.1097/MD.0000000000016408; 日本;2019
乳酸镁缓释片(magnesium lactate)
Case10:GS+低血压,28岁(20岁初孕发病),女性,生育过2胎;英国
用药:
- 镁:
- 20~25岁:甘油磷酸镁(magnesium glycerophosphate 8mmol/片) 3片/天,耐受差;
- 25岁:乳酸镁(联合 阿法骨化醇alfacalcidol),血镁0.6以后停用至今
- 钾:
- 20~25岁:Sando-K(氯化钾+碳酸氢钾,12mmol K/片)2片 x 3次/天,效果不佳;
- 25~28岁:Slow-K(氯化钾缓释片 8 mmol K/片)12~8片/天;
- 其他:
- 阿法骨化醇alfacalcidol:250 ng x3次/天 (1000ng = 1 微克 = 1/1000 毫克),主治骨质疏松,维D代谢异常(低血钙、手足抽搐等),与镁剂作用偶有高血镁报道
- vitamin D3
- (曾用药)保钾利尿剂:螺内酯、 阿米洛利,均不耐受(低血压,s 80/60 mm Hg)
效果(25~28岁):
- 血钾:3年随访均>3(3.4 某次);血镁:3年随访均 > 0.65
- 每3~4个月发作一次,一般是由于精神焦虑或传染病引起
At 20 years of age, the patient had been found tohave a persistently low serum potassium level (<3.0 mmol/L) during the second trimester of her first pregnancy ... During her second pregnancy at 22 years of age, the patient was again found to have hypokalaemia (<3 mmol/L) in association with mild hypomagnesaemia ......
Following delivery, the serum potassium level remained below the reference range. The patient was subsequently started on Sando-K, two tablets (12 mmol of potassium/tablet) three times a day, and
magnesium glycerophosphate, one tablet (8 mmol) three times a day. Despite this, she required repeated
hospital admissions (almost once a month) for symptomatic hypokalaemia with potassium levels as low as 2.1 mmol/L … …Since oral potassium supplements failed to correct her chronic hypokalaemia, she was treated with potassium-sparing diuretics, initially spironolactone螺内酯 and subsequently amiloride 阿米洛利, but she could not tolerate either as they caused hypotension. At 23 years of age, the patient underwent a genetic test, which confirmed GS as a heterozygous mutation in SLC12A3.
The patient was started on weekly intravenous infusions of potassium (40 mmol) and magnesium (10 mmol) in 1 L 0.9% saline over 8 h with a reduction in the dose of oral potassium to eight tablets a day of Slow-K. She was started on magnesium glycerophosphate, one tablet three times a day, but this was later changed to magnesium lactate one tablet three times a day, as she was intolerant to the former … preferred to have intravenous potassium and magnesium infusion a day before her menstrual period was due.
The patient has been on this protocol for 3 years, with a serum potassium level >3 mmol/L on most readings (always >2.5) and a serum magnesium level consistently >0.65 mmol/L. She has been enjoying a better physical performance level, has completed a degree in law and is in a stable job; The frequency of emergency admissions for symptomatic hypokalaemia has reduced to once every 3–4 months, and this is usually precipitated by emotional stress or infections.
Management of a severe case of Gitelman syndrome with poor response to standard treatment,2016 皇家利物浦和布罗德格林大学医院,英国,doi:10.1136/bcr-2015-212375
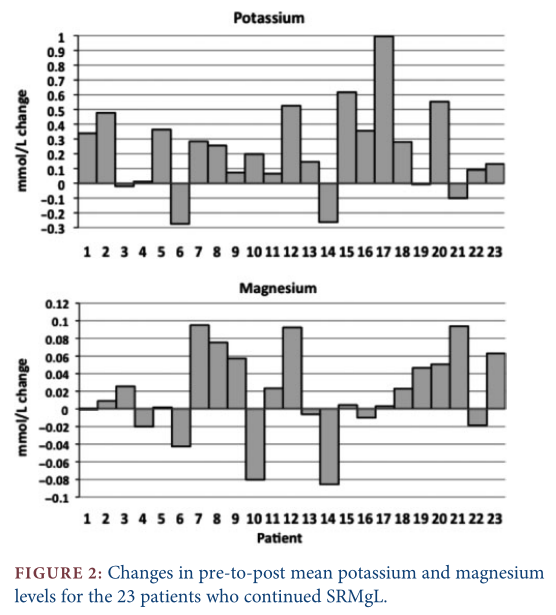
Case11:28例GS使用乳酸镁缓释片的对比试验,英国剑桥大学
We report here the analysis of a cohort of 28 adult patients with genetically proven GS who attend our specialist tubular disorders clinic, in whom we initiated the use of a modified-release Mg preparation (slow-release Mg lactate) and whowere surveyed byquestionnaire.
Results: Twenty-five patients (89%) preferred the new treatment regimen. Of these 25, 17 (68%) regarded their symptom burden as improved and seven reported no worsening. Of the 25 who were not Mg-treatment naı ¨ve, 13 (59%) patients reported fewer side effects, 7 (32%) described them as the same and only 2 (9%) considered side effects to be worse. Five were able to increase their dose without ill-effect. Overall, biochemistry improved in 91% of the 23 patients switched from therapy with other preparations who chose to continue the modified-release Mg preparation. Eleven (48%) improved both their Mg and K mean levels, 3 (13%) improved Mg levels only and in 7 cases(30%),K levelsalone rose.
Conclusions:Patient-reported and biochemical outcomes using modified-release Mg supplements were very favourable, and patient choice should play a large part in choosing Mg supplements with GS patients.
Robinson CM, Karet Frankl FE. Magnesium lactate in the treatment of Gitelman syndrome: patient-reported outcomes. Nephrol Dial Transplant. 2017;32(3):508-512. doi:10.1093/ndt/gfw019
吡咯烷酮羧酸镁(magnesium pyrrolidone carboxylate)
Case12:GS,复合杂合,26岁,男,波兰
用药:
- 吡咯烷酮羧酸镁:18 mmol/天
- 氯化钾:20 mmol/天
效果:改善(具体程度未知)
A 26-year-old male was admitted to the hospital due to incidence of syncope, generalized and muscular weakness and muscle cramps. The patient’s history revealed an episode of syncope with potassium level 3.16 mmol/l. In further follow up in outpatient assessment, recurrent incidence of hypokalemia (the lowest value 2.6 mmol/l) was observedHe received 20 mmol of potassium chloride and 18 mmol of magnesium pyrrolidone carboxylate, with clinical improvement
A case report of Gitelman syndrome resulting from two novel mutations in SLC12A3 gene,2015 http://dx.doi.org/10.1016/j.nefroe.2015.09.004;Medical University of Gdansk;波兰
镁片种类搜集及比较
参考文献(全文下载链接)
本文中提及的文献全文下载
https://pan.baidu.com/s/1hZf-4O8dH92pnqFYcX8U4g
提取码:pjkx


若有收获,就点个赞吧
0 人点赞
