本文链接:https://www.yuque.com/gs123/share/how_to_mag/
说明:
- 本文涉及的任何观点均不构成任何临床治疗建议,请咨询医生!
- 本人不是医生,以下错误之处,还请读者(特别是医学专业人士)不吝指正,谢谢。
最近更新:2020/6/7
本文部分观点缺乏文献支持,关于GS镁补充剂讨论的最新观点详见下文:
15种镁的生物利用度试验:文献摘要 + 医生点评
挑选镁补充剂的考虑因素
- 生物利用度:吸收率高,可以减少剂量,从而减少副作用
- 副作用:如果副作用大,肠道不耐受导致腹泻,会导致肠道丢失钾镁,从而可能加重低血钾、血镁
- 剂型:最好是缓释片形式(推荐 Mag Tab SR),其次是肠溶片/胶囊,因为镁的吸收部位在小肠末端和直肠,过早在胃里溶解只会增加对胃肠道刺激,对增加吸收意义不大。最常见的明胶胶囊溶解时间10-15分钟,植物纤维胶囊25-50分钟,因此植物纤维胶囊更好(https://capsuline.com/products/capsuline-clear-vegetarian-acid-resistant-enteric-coated-empty-capsules-size-0)
- 镁元素含量:含量越高,意味着药片可以做得越小,特别对于儿童服药更友好
- 镁盐的代谢产物对血气PH的影响,是否可能加重代谢性碱中毒。but,镁盐的用量(跟钾盐相比)较小,因此酸碱平衡不是最主要的考虑因素。优先考虑吸收好、副作用小的镁盐。
- 其他成分:由于市场上能买到的镁补充剂大部分是保健品,成分往往比较复杂。其他成分是否可能存在不利影响。比如说钙,GS犹豫钙的重吸收、骨密度增加,从而导致软骨钙质沉着症、骨折的风险增加,因此无需额外补钙。
各种镁盐的镁含量和生物利用度(KDIGO,2017)
| ** | ** | 镁元素% | 每克药物 含镁量(mg) |
每克药物 含镁量(mEq) |
获得50mEq需要的药物(g) | ** |
|---|---|---|---|---|---|---|
| **Gluconate | 414.6 | 6% | 55 | 5 | 11 | 19% |
| **Orotate | 334.5 | 6% | 62 | 5 | 10 | |
| **Malate | 156.4 | 7% | 65 | 5 | 9 | |
| **Aspartate | 288.5 | 8% | 84 | 7 | 7 | |
| **Glycinate | 172.4 | 9% | 90 | 7 | 7 | |
| **Sulfate | 120.4 | 10% | 100 | 8 | 6 | 4% |
| **Lactate | 202.5 | 12% | 120 | 10 | 5 | 41% |
| **Chloride | 95.2 | 12% | 120 | 10 | 5 | 20% |
| Glycerophosphate ** |
194.4 | 13% | 125 | 10 | 5 | |
| **Pidolate | 280.5 | 16% | 160 | 13 | 4 | |
| **Citrate | 214.4 | 16% | 160 | 13 | 4 | 16% |
| **Hydroxide | 58.3 | 42% | 420 | 34 | 1 | |
| **Carbonate | 84.3 | 45% | 450 | 37 | 1 | 30% |
| **Oxide | 43.3 | 60% | 600 | 49 | 1 | 4% |
生物利用度数据来自Firoz M 和Graber M. Magnes Res 2001;14:257-262; Walker AF et al. Magnes Res 2003;16:183-191; https://www.gwh.nhs.uk/media/226663/oral-magnesium-preparations-for-the-treatment-and-prevention-of-hypomagnesaemia-ukmi-qas.pdf 等网站 数据已四舍五入
文献观点摘录:
水溶解度是影响镁盐生物利用度的重要因素。有机盐的溶解度大于无机盐。枸橼酸镁比氧化镁更易吸收,血镁和尿镁检查结果均支持这一结论。
The water solubility of a Mg salt is of importance for the bioavailability. The studies demonstrate that organic salts of Mg have a higher solubility than inorganic salts. This means that Mg-citrate has a higher absorption than Mg-oxide. This is reflected in the results where the plasma concentration and urinary excretion at different times after administration were higher than for Mg-oxide. In conclusion available data suggest that Mg-citrate is the most appropriate preparation for therapeutic and supplementing purposes.
Bioavailability of Magnesium Salts Journal of Pharmacy and Nutrition Sciences, 2014 Vol. 4, No. 1
Bioavailability of Magnesium Salts – A Review.pdf
BioavailabilityofCommercialMagnesiumPreparations.pdf
尿排泄试验的结果表明,**氯化镁的吸收(生物利用度)≥ 乳酸镁 > 门冬氨酸镁 > 氧化镁**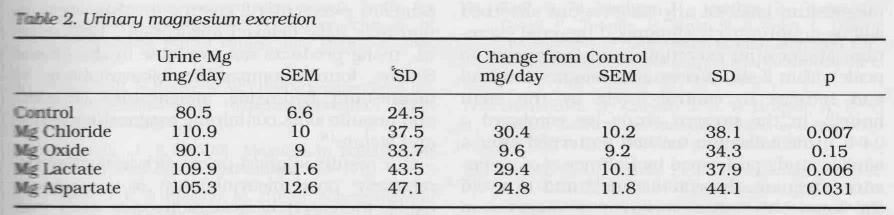
BioavailabilityofCommercialMagnesiumPreparations.pdf
Magnesium Absorption in Humans - 瑞士苏黎世理工-博士论文.pdf
氯化镁的耐受性优于硫酸镁和氧化镁
High doses of magnesium sulfate硫酸镁 or oxide氧化镁 may cause diarrhea. Magnesium chloride is better tolerated and can be used at a daily dosage of 4–5mg/kg/day divided into 3–4 doses in order to avoid diarrhea
Gitelman syndrome: pathophysiological and clinical aspects;2010 DOI: 10.1093/qjmed/hcq123
氧化镁和硫酸镁的生物利用度明显低于氯化镁、乳酸镁和天门冬氨酸镁
The bio-availability of magnesium preparations is different. Magnesium-oxide and magnesium-sulfate have a significantly lower bio-availability compared to magnesium-chloride, magnesium-lactate and magnesium-aspartate. We recommend the administration of magnesium-chloride orally to compensate for renal Mg2+ and Cl- losses. Initial daily dose is 3 mmol Mg/m2/24 hrs or 4–5 mg/kg/24 hrs. This dose should be divided in 3–4 administrations to avoid diarrhea and has to be adjusted according to serum magnesium levels. The dose usually has to be increased during periods of undercurrent infections especially those accompanied by vomiting and diarrhea. In case of acute tetany, 20% MgCl2 should be administered intravenously (0.1 mmol Mg/kg per dose) and can be repeated every 6 hours.
Gitelman syndrome,Orphanet J Rare Dis. 2008; 3: 22. ;2008 doi: 10.1186/1750-1172-3-22 ;__IF=3.687
镁盐与代谢性碱中毒
有些镁盐的阴离子代谢后会变成碳酸氢根离子(HCO3-),从而可能加重血清碱中毒……
葡萄糖盐,门冬氨酸盐,可能加重代谢性碱中毒
It is mandatory to use potassium chloride because other potassium salts, linked with poorly absorbable anions such as gluconate or aspartate, do not correct hypokalemia and can even worsen the metabolic alkalosis…
Gitelman syndrome: pathophysiological and clinical aspects;意大利,2010 DOI: 10.1093/qjmed/hcq123;IF=3.2
碳酸氢盐,乳酸盐,枸橼酸盐,醋酸盐
如果在短期内给予⼤量的碳酸氢钠(或任何可代谢形成碳酸氢盐的有机阴离⼦钠盐,如乳酸钠、枸橼酸钠或醋酸钠),可能会出现更严重的代谢性碱中毒……使⽤⼤量枸橼酸盐可导致代谢性碱中毒。输⾎量超过8个单位时有可能出现该情况。⽤于⾎液抗凝的枸橼酸及枸橼酸钠,随后经代谢形成碳酸氢钠。
代谢性碱中毒患者补充钾盐时,氯化钾是⾸选制剂(是否可以推论:氯化镁是首选补镁剂?)。如有可能,应避免使⽤有机阴离⼦钾盐,如枸橼酸盐或醋酸盐,因为这些阴离⼦代谢会产⽣碳酸氢盐,从⽽减慢代谢性碱中毒的纠正速率。 《代谢性碱中毒的成因》《代谢性碱中毒的治疗》Uptodate临床顾问
理解gitelman碱中毒的成因,可以帮助我们理解和消除在钾镁补充剂使用中,对碱中毒的担忧。
- 成因:电解质的平衡,根本的原因是肾小管对氯离子的重吸收减少(所以尿氯升高),从而使
食补:富含镁的食物,及其葡萄糖、钾和卡路里含量
https://www.yuque.com/gs123/share/kdigo2016_gitelman_syndrome#lenPO
参考文献(全文下载链接)
本文中提及的文献全文下载
https://pan.baidu.com/s/1hZf-4O8dH92pnqFYcX8U4g
提取码:pjkx


若有收获,就点个赞吧
0 人点赞
